You’ve seen the movies. Someone gets a tiny scratch on their neck and suddenly there’s a geyser of red. Hollywood loves the drama, but honestly, they usually get the anatomy totally wrong. Most people use the terms interchangeably, thinking any pipe in the neck is just a "vessel," but the carotid and jugular vein are about as different as a high-pressure fire hose and a slow-moving drainage pipe. If you don't know which is which, you're missing the basic blueprint of how your brain actually stays alive.
Let's get the big one out of the way first. The carotid is an artery. The jugular is a vein. That might sound like a "well, duh" medical distinction, but it changes everything about how your body handles pressure, oxygen, and injury. Arteries like the carotid are the delivery trucks. They are thick-walled, muscular, and carrying blood that was just blasted out of your heart at high velocity. Veins, like the jugular, are the return service. They’re thinner, under much lower pressure, and basically just let gravity do the heavy lifting to get "used" blood back down to the lungs and heart.
The High-Pressure Highway: Understanding the Carotid Artery
When you feel for a pulse on the side of your neck, you aren't feeling your jugular. You’re feeling the common carotid artery. This thing is a beast. It branches off from the aorta—the body's main power line—and heads straight for the skull. Evolution didn't take any chances here; the brain is an energy hog, consuming about 20% of your body's oxygen despite being a tiny fraction of its weight. To keep that engine running, the carotid provides a constant, forceful stream of oxygenated blood.
Why location matters
The carotid isn't just one tube. It splits. Around the level of your "Adam's Apple" (the thyroid cartilage), it bifurcates into the internal and external carotid. The internal goes deep, feeding the brain itself. The external stays "outside," providing blood to your face, scalp, and jaw. This is why a scalp wound bleeds so much—it’s getting a direct feed from a high-pressure line.
Interestingly, at that split point, there’s a little bundle of nerves called the carotid sinus. It acts like a built-in blood pressure monitor. If your pressure spikes, the sinus senses the stretch in the artery wall and tells your heart to slow down. It’s a delicate balance. Medical students are often taught about "Carotid Sinus Hypersensitivity," where even a tight collar or a quick turn of the head can accidentally trigger this sensor, causing a person to faint because the body "thinks" the blood pressure is too high when it’s actually totally fine.
The Gravity Feed: What the Jugular Actually Does
While the carotid is pushing blood up, the carotid and jugular vein work in a loop, and the jugular's job is the cleanup. There are actually two main sets: the internal and external jugular veins. Most people don't realize that the internal jugular is actually much larger and more important than the one you can sometimes see popping out when someone is shouting or lifting weights.
The internal jugular vein (IJV) is the primary exit route for blood leaving the brain. It sits right next to the carotid artery, tucked under a large muscle called the sternocleidomastoid. It’s huge—roughly the diameter of your thumb in some spots—but the walls are thin. Why? Because it doesn’t need to withstand pressure. It just needs to be a wide-open pipe.
- The Internal Jugular: Hidden deep, handles the bulk of the drainage.
- The External Jugular: This is the "angry vein" you see on a singer’s neck. It drains the scalp and face.
- Pressure Dynamics: Unlike the carotid, the pressure in the jugular is often negative relative to the atmosphere when you’re standing up. This is because gravity is pulling the blood down so effectively.
This negative pressure is actually a bit of a safety hazard. If the jugular is cut while a person is upright, the vein doesn't always spray blood out; sometimes, it sucks air in. This is called an air embolism. If enough air gets sucked into the vein, it can travel to the heart and literally lock the pump, stopping blood flow entirely. This is why paramedics are so aggressive about sealing neck wounds with airtight dressings—it’s not just about stopping the bleed; it’s about stopping the "suck."
Why Surgeons Worry About the Carotid-Jugular Relationship
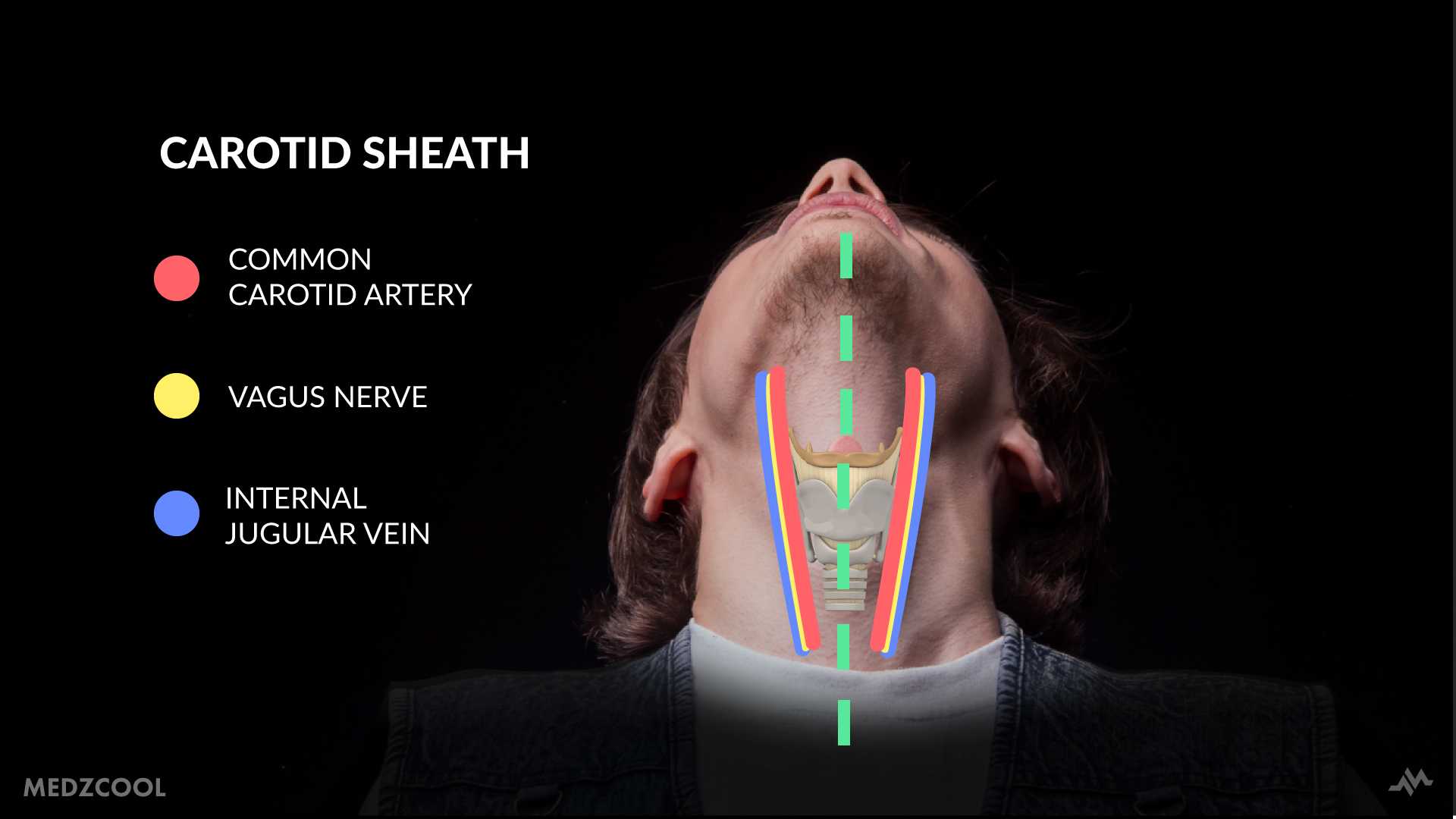
If you're ever in a position where a doctor is poking around your neck—say, for a thyroid surgery or a carotid endarterectomy—they are walking a tightrope. These two vessels are bundled together in something called the carotid sheath. It’s a tube of connective tissue that also holds the vagus nerve, which controls your heart rate and digestion.
They are packed so tightly that an issue with one often impacts the other. For example, if someone has "Jugular Venous Distension" (JVD), where the vein stays bulging even when they are sitting up, it’s a massive red flag for heart failure. It means the right side of the heart is backed up, and the "drainage pipe" is getting full because it has nowhere to dump its load.
The Carotid Plaque Problem
On the flip side, the carotid faces the "clogged pipe" issue. Because of the high pressure and the way the vessel forks, it’s a prime spot for cholesterol and calcium to build up. This is Carotid Artery Disease. If a piece of that "gunk" (plaque) breaks off, it goes straight to the brain. That’s a stroke. According to the Journal of the American Heart Association, carotid stenosis is a leading cause of ischemic strokes worldwide. Surgeons often have to go in and literally "roto-rooter" the artery out, a procedure called an endarterectomy, to prevent a catastrophic blockage.
Real World Dangers: Distinguishing Injuries
Let’s talk about trauma. It’s a grim topic, but knowing the difference between a carotid and jugular vein injury is literally the difference between life and death.
An arterial bleed (carotid) is pulsatile. It spurts in time with the heartbeat. The blood is bright red because it is rich in oxygen. This is a "minutes to live" situation because the brain is being deprived of its primary fuel source while the body’s total blood volume drops rapidly.
A venous bleed (jugular) is different. The blood is darker—almost a deep maroon or purple—because it has already dropped off its oxygen. It doesn't spurt; it flows. It looks like a heavy, steady leak. While still incredibly dangerous, it’s often easier to control with direct pressure than a high-pressure arterial rupture.
- Direct Pressure: For either vessel, you push hard. You don't "check" to see if it stopped.
- The Air Factor: With the jugular, you must keep the person lying flat or even with their head slightly lower than their heart to prevent air from being sucked into the vein.
- The Pulse Check: Never press on both carotids at once. You can accidentally trigger that carotid sinus reflex we talked about, causing the heart rate to drop dangerously low or cutting off blood to the brain entirely.
Common Misconceptions and Nuance
People often think the "jugular" is the most vulnerable part of the neck. In reality, the carotid is much more "important" for immediate survival. You can actually have one jugular vein completely blocked or removed (sometimes done in radical neck dissections for cancer) and the other side will usually pick up the slack. Your body is surprisingly redundant with its drainage.
However, you cannot just "lose" a carotid. If one carotid is blocked, the other side tries to compensate via a circular network of vessels at the base of the brain called the Circle of Willis. But not everyone has a "complete" Circle of Willis. Some people are born with gaps in this backup system, making them much more vulnerable to a carotid blockage. It’s one of those weird anatomical quirks that you never know you have until you need it.
A Note on Modern Medicine
We've gotten really good at fixing these pipes. Interventional radiologists can now thread a catheter from your groin all the way up to your neck to put a stent in a narrowing carotid. They don't even have to "cut" the neck anymore in many cases. We also use the internal jugular for "Central Lines"—if a patient is very sick, doctors will put a large IV directly into the jugular because it leads straight to the heart, allowing for rapid medication delivery.
Assessing Your Own Health
You don't need a medical degree to keep an eye on your neck health, but you do need to be aware of the signals. Most carotid issues are silent until they aren't.
- Listen for "Bruits": Doctors use a stethoscope to listen to the carotid. If they hear a "whooshing" sound (a bruit), it means the blood flow is turbulent, usually because of a blockage.
- Watch for TIA: A Transient Ischemic Attack is a "mini-stroke." If you have sudden weakness on one side or slurred speech that goes away in ten minutes, that’s your carotid telling you it's about to fail.
- Check for Bulges: If your jugular vein is bulging while you're standing or sitting upright, it’s time to see a cardiologist. Your "drainage system" shouldn't be backed up like that.
Actionable Steps for Vascular Health
Maintaining the integrity of the carotid and jugular vein isn't about some "magic" neck exercise. It's about systemic plumbing maintenance.
- Manage Blood Pressure: High pressure "bangs" against the walls of the carotid, causing micro-tears that the body repairs with plaque. Keep your numbers below 120/80.
- Stop Smoking: This isn't just for your lungs. Nicotine and the chemicals in smoke physically damage the lining of your arteries (the endothelium), making it "sticky" for cholesterol.
- Neck Protection: If you play contact sports like hockey or participate in martial arts like Brazilian Jiu-Jitsu, understand the risks of carotid artery dissection. A sudden, violent snap of the neck can tear the inner lining of the artery, leading to a clot. Wear a neck guard if the sport allows it.
- Get an Ultrasound: If you’re over 65 or have a history of smoking and high blood pressure, a simple, non-invasive carotid ultrasound can see exactly how much "gunk" is in your pipes before it becomes a problem.
Basically, treat your neck with some respect. It's a crowded neighborhood where the most important "wires" in your body are all shoved into a very small, unprotected space. Knowing the difference between the supply line (carotid) and the return line (jugular) is just the first step in making sure the whole system stays pressurized and flowing correctly.
Keep your blood pressure in check and listen to what your body is telling you. If you feel a "thumping" or see a new bulge, don't wait for a movie-style "geyser" to take it seriously. Go get it checked out by a professional who knows the difference between a delivery truck and a drain.